
Were Covid Patients Put on Ventilators to Maximize Hospital Profits?
Executive Summary
- US Hospitals were given a strong financial incentive to place covid patients on ventilators.
- How much did this result in people being placed on ventilators that received no benefit?
Introduction
During the height of the COVID pandemic, there were constant conversations about ventilators and the shortage of ventilators. It has been discussed that ventilators don’t do much for covid patients. I then learned that Medicare paid $39,000 for every patient on a ventilator. This raises the question of whether patients were placed on ventilators because it was an appropriate treatment or profit-maximizing for the hospitals.
Our References for This Article
To see our references for this article and related Brightwork articles, visit this link.
What Was the Impact of Hospitals on Covid?
The lockdowns were partly justified by the idea that hospitals had a critical role in responding to the pandemic. This was encapsulated in the often-repeated logic of “flattening the curve.”
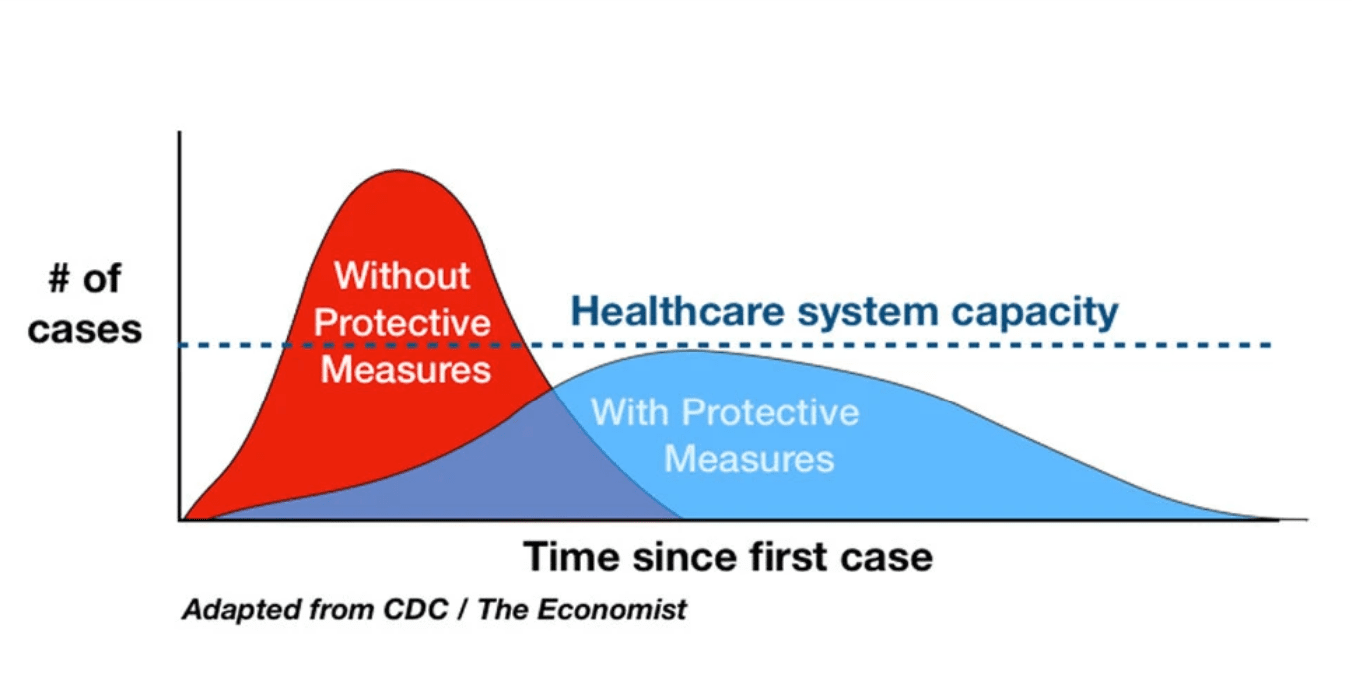
This graphic was repeatedly used to promote the lockdown and was based on not overstressing the healthcare system. However, this implies that hospitals had effective treatments for patients. This assumption turned out not to be true.
- If one recalls, the focus was not using the health care system to deal with covid cases.
- This policy was ineffective because most medical systems (like putting people on ventilators) did not work.
- Hospitals treated many people, but they did not do much for them. As is usually the case, the medical system took full credit for people who recovered through their bodies’ natural immune systems.
- Hospitals began draping themselves in glory and routinely stated that “heroes” worked at these hospitals.
What Could Hospitals Do for Covid Patients?
The following is a comment on a New York Times article.
I mean, as a doc dispatched to COVID ICUs for the last many months, it’s rather misleading to insinuate that coming to hospital is some magic bullet here. Our mainstay of treatment at this point is “supportive care” essentially a fancy word for babysitting the patient and hoping they recover. It also includes emergency procedures such as intubation to “support” patients though particularly challenging phases of the disease. And there are at this point unsubstantiated treatments including steroids, anti inflammatories like tocilizumab, and convalescent plasma, all with weak evidence supporting them and none of which have proven efficacy in a gold standard blinded clinical trial. Obviously the example in the lead where the poor man is already in respiratory failure is different, but I’d hardly call it the standard and the benefits avoiding hospital if at all possible has been since day 1 and continues to be excellent advice in this setting. – NYT
This graphic was repeatedly used to promote the lockdown and was based on not overstressing the healthcare system. However, this implies that hospitals had effective treatments for patients. This assumption turned out not to be true.
- If one recalls, the focus was not using the health care system to deal with covid cases.
- This policy was ineffective because most medical systems (like putting people on ventilators) did not work.
- Hospitals treated many people, but they did not do much for them. As is usually the case, the medical system took full credit for people who recovered through the natural immune systems of their bodies.
- Hospitals began draping themselves in glory and routinely stated that “heroes” worked at these hospitals.
What Could Hospitals Do for Covid Patients?
The following is a comment on a New York Times article.
I mean, as a doc dispatched to COVID ICUs for the last many months, it’s rather misleading to insinuate that coming to hospital is some magic bullet here. Our mainstay of treatment at this point is “supportive care” essentially a fancy word for babysitting the patient and hoping they recover. It also includes emergency procedures such as intubation to “support” patients though particularly challenging phases of the disease. And there are at this point unsubstantiated treatments including steroids, anti inflammatories like tocilizumab, and convalescent plasma, all with weak evidence supporting them and none of which have proven efficacy in a gold standard blinded clinical trial. Obviously the example in the lead where the poor man is already in respiratory failure is different, but I’d hardly call it the standard and the benefits avoiding hospital if at all possible has been since day 1 and continues to be excellent advice in this setting. – NYT
The mortality rate of covid patients placed on ventilators and intubated is high. One primary reason is that intubation dramatically reduces the immune system, as the lymphatic system requires body movement to obtain lymphatic circulation. Naturally, the body needs all of its immunity. Furthermore, those who come off the ventilator can have breathing problems due to being on the ventilator. The overuse of ventilators is explained in the following quotation.
Recognizing this, some intensive care units have started to delay putting a COVID-19 patient on a ventilator to the last possible moment, when it is truly a life-or-death decision, said Dr. Udit Chaddha, an interventional pulmonologist with Mount Sinai Hospital in New York City. – WebMD
And this quotation.
Starting this month, a few physicians have voiced concern that some hospitals have been too quick to put Covid-19 patients on mechanical ventilators, that elderly patients in particular may have been harmed more than helped, and that less invasive breathing support, including simple oxygen-delivering nose prongs, might be safer and more effective.
“This is one of the first coherent, comprehensive, and reasonably clear discussions of the pathophysiology of Covid-19 in the lungs that I’ve seen,” said palliative care physician Muriel Gillick of Harvard Medical School, who was one of the first to ask if ventilators were harming some Covid-19 patients, especially elderly ones.
There is a growing recognition that some Covid-19 patients, even those with severe disease as shown by the extent of lung infection, can be safely treated with simple nose prongs or face masks that deliver oxygen.
Earlier this month, the Mount Sinai Health System in New York developed a protocol to repurpose sleep apnea machines for Covid-19 patients, while in Rhode Island, the Department of Public Health, University of Rhode Island, and others are collecting the devices for hospitals to use instead of ventilators where possible.
The Covid-19 treatment guidelines released by the NIH do not specifically address what criteria physicians should use for putting patients on a ventilator. But in a recognition of the damage that the ventilators can do, they recommend a phased approach to breathing support: oxygen delivered by simple nose prongs, escalating if necessary to one of the positive-pressure devices, and intubation only if the patient’s respiratory status deteriorates. If mechanical ventilation becomes necessary, the NIH said, it should be used to deliver only low volumes of oxygen, reflecting the risk of damaging healthy lung tissue. – StatNews
And this one.
some critical care physicians are questioning the widespread use of the breathing machines for Covid-19 patients, saying that large numbers of patients could instead be treated with less intensive respiratory support.
If the iconoclasts are right, putting coronavirus patients on ventilators could be of little benefit to many and even harmful to some. – StatNews
Conclusion
It is unclear how much the money paid by Medicare promoted ventilators for those with covid. There is good evidence that ventilation intubation was vastly overused, and there is no good evidence that intubation helps. Some drugs like Ivermectin and various vitamins that have been shown to reduce the impact of COVID-19 were not used at hospitals and continue not to be used at hospitals to treat COVID-19. This again brings up how much hospitals base their treatments on evidence versus the pharmaceutical-controlled narrative. Secondly, it is difficult to imagine that the extra revenues from placing covid patients on ventilators did not impact the decision.
Addressing the Damage
One of the best ways to address the damage caused by the covid vaccines is with Ivermectin. This is the reason I began taking Ivermectin -- before investigating all the other health benefits of the drug. Now, I take Ivermectin for many reasons.
- We have Ivermectin dosage calculators based on research studies and for all the different uses of Ivermectin.
- We are the only web source offering an Ivermectin dosage calculator in addition to different dosage estimates for different cancer types.
- All of our calculators are easy to use (see our dosage calculator listing). Each person enters their personalized information into the calculator and receives our recommended extensively researched dosage estimate automatically and immediately calculated.
- We also cover the broader problems with dosage calculation in medicine at the article The Problem With Dosage Calculation in Medicine, as this is an issue much larger than for one drug.
About Our Ivermecting Testing Program and Recommended Ivermectin Source of Supply
- We performed pharmaceutical testing on Ivermectin to find a lower-cost version that also matched Merck's original Ivermectin in bioequivalence.
- You can read about the details of our Ivermectin testing in this article, Our Ivermectin Bioequivalence Testing.
- We got Summit Products to carry this version of Ivermectin, which passed our bioequivalence testing.